


TDD #21: Two Georgia Woman Die After Taking Abortion Pills
What happened and who's to blame?

Welcome to another edition of The Dobbs Digest, a newsletter of Confessions of a Truthaholic.
Abortion may be the most most divisive and intractable topic in contemporary American politics. And the inflammatory rhetoric, which reached boiling point after Roe v. Wade was overturned in the summer of 2022, isn’t simmering down anytime soon. But most of what I read and hear is sky high on emotion but low on facts, so bear that in mind as you scroll.
My sole purpose with this newsletter is to question the assumptions of the media narratives shaping abortion discourse and to unpack the actual issues raised in the courts to get us to a shared understanding of the reality on the ground.
If you’re new to this newsletter, please read our welcome post here so you’re in the know. So glad to have you here.

Two Georgia Women Die After Taking Abortion Pills
ProPublica recently published a pair of articles featuring stories of two Georgia women, Amber Nicole Thurman and Candi Miller, who passed away after taking legally obtained and FDA-approved chemical abortion pills. These deaths were horrific, tragic, and, based on various reports, preventable. I agree.
But the ProPublica stories aren’t about the risks of chemical abortion - specifically self-managed, or DIY, chemical abortion - they’re hit pieces blaming former President Trump for the deaths of these two women and their gestating children, including a set of twins.
ProPublica argues that:
Trump is personally responsible for overturning Roe v. Wade, so …
Trump is personally responsible for any-and-all resulting post-Dobbs state legislation (statutes) restricting abortion, aka “Trump abortion bans,” and therefore …
Trump is personally responsible for the deaths of Amber Nicole Thurman and Candi Miller because of these statutes (particularly Georgia) prevented them from getting life-saving medical care.
In sum, ProPublica claims that but for these “abortion bans,” Amber and Candi would be alive today.
Is their claim true or is it false?
SIDEBAR » While I’m never surprised by progressive ProPublica pieces that seek to smear, defame, and attack conservatives and conservative positions (they’re leading the anti-Clarence Thomas campaign), I was a little surprised by the angle these articles took while trying to pin these tragic abortion-related deaths onto Georgia’s abortion statute. I expected some spin, but I was shocked they actually tried to make a causal link between the current Georgia law and these deaths without quoting, citing, or even referencing it - they simply call it the “new Georgia law” and then proceed to lie about its contents. Additionally, they conveniently ignored the federal rules and regulations governing abortion, specially chemical abortions, that are established by and implemented within the executive branch of government, i.e. the FDA Department of Health and Human Services.
Before we investigate ProPublica’s claim, let’s get on the same page with some legal preliminaries.
Self-managed, or do-it-yourself (DIY), abortion is legal in all 50 states.
Performing an abortion to preserve the life of the mother is legal in all 50 states.
Whether the mother’s life is in danger is determined in the sole discretion of the physician performing the abortion.
Women are not subject to criminal prosecution or civil liability in any state for having an illegal abortion. In the few cases where post-abortive women have been investigated, it’s been for a separate crime, such as illegal disposal of human remains, NOT for having an abortion.
All federal and state abortion laws and regulations are directed toward abortion providers, not women having abortions.
Shield laws further protect abortion pill providers from civil liability and adverse insurance claims for mailing abortion pills to particular states
With that out of the way, let’s take a look at ProPublica’s claims.
The Reported Facts
Both Amber and Candi legally obtained pills for chemical abortion, which include two drugs: the first, Mifeprex (generic name “mifepristone”) and the second, Cytotec (generic name “misoprostol”).
Both women took the first drug, mifepristone. Candi took it at home in Georgia, Amber took it at a medical clinic in North Carolina.
Both women took the second drug, misoprostol, at home in Georgia.
Both women had incomplete abortions, meaning that some of the pregnancy tissue remained in the womb after the fetus and other products of conception were discharged from the uterus.
Both women experienced severe pain and both after their abortions delayed seeking medical care.
Both women contracted infections as a result of their incomplete abortions and both women died.
Amber Thurman died from sepsis. Candi Miller’s specific cause of death hasn’t been released since the autopsy revealed the presence of numerous other drugs, including various painkillers and fentanyl, in addition to infected human remains in her womb. It’s unclear whether she died from the infection or the unrelated drugs.
CONCLUSION #1:
Both women had legal self-managed medication abortions and both women died from complications arising from those abortions.
Some background on abortion pills …
What is Chemical Abortion?
Chemical abortion is a two-drug cocktail taken within 24 - 48 hours of each other.
Drug #1: Mifeprex / Mifepristone
First, a pregnant woman takes Mifeprex (formerly known as RU-486 and now referred to with the generic term mifepristone), which is a synthetic hormone that stops the production of progesterone. Progesterone is required to build the uterine lining, which is required for the fetus to receive nutrition and develop in the womb. By blocking progesterone, mifepristone causes chemical destruction of the uterine lining, resulting in withdrawal of nutrition and fetal demise.
Drug #2: Misoprostol
Second, within 24 - 48 hours of taking mifepristone, the pregnant woman completes the abortion by taking misoprostol (this is the generic name for Cytotec). Misoprostol causes the uterus to contract, cramp, and push out the uterine lining, which includes the expired fetus and related pregnancy tissue. It mimics a very heavy menstrual cycle. While mifepristone is what terminates the pregnancy and can technically be taken alone, it only works in isolation in less than 25% of chemical abortions, hence the need for misoprostol. If any pregnancy tissue remains for a period of time (from days to weeks), it will become infected and require immediate treatment.
Mifeprex / Mifepristone also comes with the following black box warning.
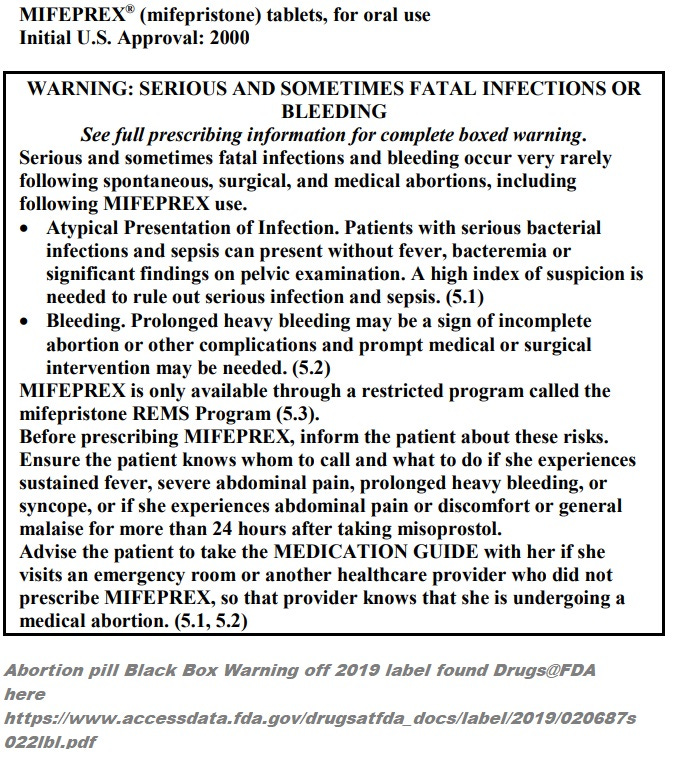
Make note of the fact that mifepristone is only available through a restricted program called the Mifeprex REMS Program (Risk Evaluation and Mitigation Strategies). So, the REMS is very important!

What is the Mifeprex REMS?
REMS stands for Risk Evaluation and Mitigation Strategy (REMS). Per the FDA, REMS is a …
“drug safety program that the U.S. Food and Drug Administration (FDA) can require for certain medications with serious safety concerns to help ensure the benefits of the medication outweigh its risks. REMS are designed to reinforce medication use behaviors and actions that support the safe use of that medication. While all medications have labeling that informs health care stakeholders about medication risks, only a few medications require a REMS.”
Mifeprex was originally approved by the FDA in 2000, which approval included a REMS program. Here’s a summary of the original REMS and some of the major changes made between then and the present.
Required three office visits by the patient:
Appointment 1: 600 mg of Mifeprex administered to the patient by the physician or under the supervision of the physician in a clinic, medical office, or hospital, provided the patient is not carrying a fetus more than 49 days in gestation, or approximately 7 weeks, which is confirmed via ultrasound.
Appointment 2: Patient returns on three days later for an examination with her physician; if termination of pregnancy is not complete, the physician administers 400 mcg of misoprostol, which is taken orally at the doctor’s office.
Appointment 3: Patient returns to her physician for follow up visit approximately 14 days after administration of Mifeprex to confirm complete termination of the pregnancy occurred, again, confirmed via ultrasound.
Revised Requirements (2016):
Required one office visit by the patient:
Appointment 1: 200 mg of Mifeprex (note change of dosage) administered to the patient by a qualified healthcare provider (physicians and nurse practitioners were now authorized prescribers) or under the supervision of a qualified healthcare provider in a clinic, medical office, or hospital, provided that the patient isn’t carrying a fetus of more than 70 days, or 10 weeks gestation (note increase in gestational age). The prescribing provider is to discuss an appropriate location for the patient to self-administer the second drug, misoprostol, during this appointment.
No Appointment Required: Patient takes 800 mcg of misoprostol buccally (placed in cheek) 24 - 48 hours after taking Mifeprex. Since there is no office visit requirement, patients usually administer the misoprostol at home.
No Appointment Required: Patient should (but is not required to) follow up with the prescribing provider approximately 7 - 14 days after administration of Mifeprex to (1) confirm the pregnancy has been fully terminated, and (2) to evaluate the degree of bleeding and any other side effects.
In summary, the 2016 revisions eliminated the following from the original REMS:
the 49 day / 7 week gestational period for FDA-approved use of mifepristone was enlarged to 70 days / 10 weeks
the in-person dispensing requirements at a doctor’s office; the patient could now pick up the second drug, misoprostol, at a local pharmacy for home administration
an initial ultrasound to confirm the gestational age of the fetus (Mifeprex is increasingly dangerous as the pregnancy progresses and is absolutely NOT approved for ectopic or extra-uterine pregnancies
post-abortion ultrasound to confirm a complete abortion
safeguards to ensure there aren’t any contraindications for Mifeprex (reasons a woman shouldn’t take it due to dangerous or deadly side effects given other medications she takes, such as anticoagulants, or because she has a certain blood type, diabetes, high blood pressure, etc.)
the requirement that only medical doctors could prescribe chemical abortion drugs
the requirement for reporting non-fatal complications from use of chemical abortion drugs - unless the mother dies, all reporting requirements are eliminated
Some effects of these eliminations …
The requirements of the Federal Food Drug and Cosmetic Act (FFDCA) and the Pediatric Research Equity Act (PREA) are outright ignored. These laws require safety assessments when changes are made to the REMS for drugs used by adults and children. The safety assessment should check to see how the 2016 changes to dosage, delivery (buccal v. oral), and gestational age, affect the bodies of young girls (under 18) versus adult women and whether pediatric labeling is necessary.
Without multiple touchpoints with a personal healthcare provider, women must go to their closest Emergency Room if they experience complications. It is also the patient’s sole responsibility to disclose that they’re having a medical abortion as opposed to a natural miscarriage and to provide any background medical information to the providers.
Note: In 2019, the generic form of Mifeprex, mifepristone, was approved by the FDA, so the term mifepristone is now used almost exclusively in the medical literature and FDA documentation.
Partial Suspension of 2016 REMS (2021)
2021: In April 2021, given the COVID-19 pandemic, the Biden/Harris Administration issued issued a temporary “Non-Enforcement Decision” of the 2016 REMS in-person dispensing requirements. This meant that abortion providers would no longer need to see or examine patients in person prior to prescribing abortion pills; telehealth (phone or video) appointments were now sufficient.
The Administration also temporarily suspended enforcement of federal postal service laws declaring that “[e]very article or thing designed, adapted, or intended for producing abortion … is nonmailable matter…” (18 U.S.C. §§ 1461, 1462), opening the door for mifepristone to be dispensed through the mail. This “Non-Enforcement Decision” was intended to be temporary in order to address the extraordinary circumstances of the pandemic, but …
2021: In December 2021, the Biden/Harris Administration made the “Non-Enforcement Decision” permanent, making at-home abortion legal nationwide.
SIDEBAR » Making the Non-Enforcement Decision permanent triggered the most recent litigation against the FDA which was filed by numerous physicians and medical associations who feared the suspended REMS would lead to an increase in unaddressed complications from self-managed abortion, including preventable death. Regrettably, the Biden/Harris Administration and the press characterized the litigation as a purely political move by the right to decrease abortion access, dismissing the safety claims as pretext. The Administration doubled-down and stated that the suing physicians must be defeated at all costs (formal statement referenced below). Ultimately, the case made it to the U.S. Supreme Court, but the high court dismissed it in June 2024 on technical legal grounds, claiming the physicians and associations who brought the case didn’t have sufficient standing to sue among other procedural issues arising from both sides of the case. The Court did not rule on the merits of the case so the Non-Enforcement decision remains in effect. Because the Non-Enforcement decision was an Executive Order, as opposed to legislation, it may be modified by a future administration.
For some additional context, here’s what the Charlotte Lozier Institute had to say about the suspended REMS.
“The decision by the U.S. Food and Drug Administration to suspend certain Risk Evaluation and Mitigation Strategies (REMS) for distribution of the abortion pill regimen is both unnecessary and medically unsound. The immediate impact of the decision will be to deprive women of vital medical information about their pregnancy and the health consequences of the mifepristone-misoprostol combination, which, international and domestic studies have shown, are associated with elevated rates of medical complications and emergency room visits when compared with surgical abortion. By focusing solely on COVID-19 infection and a handful of biased studies conducted since the beginning of the pandemic, the FDA’s abdication of full enforcement of the REMS ignores an array of profound concerns.”
You can read the Institute’s full statement on the issue here.
CONCLUSION #2:
More than a year before Roe v. Wade was overturned on June 24, 2022, the Biden/Harris Administration suspended elements of the 2016 Mifeprex REMS in order to legalize mail-order abortion nationwide.

The Biden/Harris Administration’s Statement on the Suspended REMS
On March 7, 2024, the Biden/Harris administration released a Fact Sheet regarding their continued “fight for reproductive freedom,” in light of the ongoing litigation against the FDA.
Here’s an important excerpt (note that the italics and bold text, except for headers, are added by me for emphasis):
[Section of Fact Sheet]
Protect Access to Abortion, Including FDA-Approved Medication Abortion
The Administration will continue fighting to protect a woman’s ability to access abortion care, including by defending access to FDA-approved, safe and effective medication abortion.
The Administration will continue to:
Protect Access to Safe and Legal Medication Abortion. On what would have been the 50th anniversary of Roe v. Wade [January 22, 2023], President Biden issued a Presidential Memorandum directing agencies to consider further efforts to support patients, providers, and pharmacies who wish to legally access, prescribe, or provide medication abortion. This Presidential Memorandum followed independent, evidence-based action taken by the Food and Drug Administration (FDA) to allow mifepristone to be prescribed by telehealth and sent by mail as well as to enable interested pharmacies to become certified to dispense the medication. As a result of the new pathway established by FDA, many pharmacies across the country—including major retail pharmacy chains—are now certified to dispense medication abortion. This new option gives many women the option to pick up their prescription for medication abortion at a local, certified pharmacy just as they would for any other medication.
Defend FDA Approval of Medication Abortion in Court. FDA and the Department of Justice (DOJ) are defending access to mifepristone—a safe and effective drug used in medication abortion that FDA first approved more than 20 years ago—and FDA’s independent, expert judgment in court, including in a lawsuit before the Supreme Court that attempts to curtail access nationwide.
SIDEBAR » This refers to the above-referenced litigation against the FDA seeking a judgment requiring them to reinstate the original Mifeprex REMS, or, in the alternative, the revised 2016 REMS, to help manage the explosion of self-managed abortion.
The Administration will continue to stand by FDA’s decades-old approval and regulation of the medication as well as FDA’s ability to review, approve, and regulate a wide range of prescription medications. Efforts to impose outdated restrictions on mifepristone would limit access to this critical medication in every state in the country.
CONCLUSION #3:
The Biden/Harris Administration celebrates it’s decision to legalize self-managed abortion nationwide by removing in-person examination and dispensing protocols included in the 2016 Mifeprex REMS.
Where Do Things Stand Now?
As a result of the 2021 Non-Enforcement decision, abortion pills are widely available online and DIY abortion is quickly rising in popularity in the United States. The website AbortionFinder.org includes a national database for in person and online abortion providers. Shield laws protect these providers from potential civil liability or adverse insurance claims for mailing mifepristone to any state, regardless of their abortion laws. Make no mistake, the abortion pill market is wide open.
CONCLUSION #4:
Self-managed abortion is legal, easy-to-obtain, and widely available nationwide.

Enter Georgia’s Abortion Law: The LIFE Act (HB 481)
Here’s the relevant language from the Living Infants Fairness and Equality (LIFE) Act …
No abortion is authorized or shall be performed if an unborn child has been determined to have a 'detectable human heartbeat,' which means embryonic or fetal cardiac activity or the steady and repetitive rhythmic contraction of the heart within the gestational sac, unless there is a medical emergency, medically futile pregnancy, [or the unborn child was conceived through rape or incest and is no further than 20 weeks].
Definitions of bolded terms from the statute …
'Abortion' means the act of using, prescribing, or administering any instrument, substance, device, or other means with the purpose to terminate a pregnancy with knowledge that termination will, with reasonable likelihood, cause the death of an unborn child; provided, however, that any such act shall not be considered an abortion if the act is performed with the purpose of removing a dead unborn child caused by spontaneous abortion; or removing an ectopic pregnancy.
'Medical emergency' means a condition in which an abortion is necessary in order to prevent the death of the pregnant woman or the substantial and irreversible physical impairment of a major bodily function of the pregnant woman. No such greater risk shall be deemed to exist if it is based on a diagnosis or claim of a mental or emotional condition of the pregnant woman or that the pregnant woman will purposefully engage in conduct which she intends to result in her death or in substantial and irreversible physical impairment of a major bodily function.
A physician determines, in reasonable medical judgment, and in their sole discretion, whether a medical emergency exists.
'Medically futile' means that, in reasonable medical judgment, an unborn child has a profound and irremediable congenital or chromosomal anomaly that is incompatible with sustaining life after birth.
A physician determines, in reasonable medical judgment, and in their sole discretion, whether a pregnancy is medically futile.
In sum …
Performing an abortion in Georgia is legal until a fetal heartbeat is detected.
Performing an abortion in Georgia is legal at any time to prevent the death of the pregnant woman or the substantial and irreversible physical impairment of a major bodily function.
Performing an abortion in Georgia is legal if the unborn child has a profound and irremediable congenital or chromosomal anomaly that is incompatible with sustaining life after birth.
Performing a dilation and currettage (D&C) procedure is legal in Georgia, unless it is for the sole purposes of performing an illegal abortion, i.e. healthy mom and healthy baby after a heartbeat is detected. D&C procedures are actually routine for miscarriage, post-abortion care, and many other gynecological issues.
Self-managed abortion is legal in Georgia.
Seeking medical help in an ER, or other physician’s office, during the course of a self-managed abortion is absolutely legal.
FYI - A close friend of mine, Dr. Janet Davis, is a Board-Certified OBGYN in Georgia specializing in maternal-fetal medicine and high-risk pregnancies. She’s practiced since 1986. I routinely reach out to her to make sure I’m not getting ahead of my skis while talking about these issues, including with respect to the claims above. Dr. Davis routinely provides emergency care to women in Georgia experiencing complications from mifepristone, largely for failing to follow the instructions for proper use. Given the modified REMS, non-fatal complications are no longer reportable so it’s impossible to collect useful and reliable data regarding drug safety.
CONCLUSION #5:
Georgia law expressly authorizes the provision of care to a pregnant woman experiencing a medical emergency as determined in the sole discretion of the physician. Georgia law also expressly releases women who have abortions from any-and-all civil and criminal liability, regardless of abortion method used.
How Could this Horrible Tragedy Happen?
Amber Thurman and her twins.
Amber was a young single mom pregnant with twins who missed her surgical abortion appointment in North Carolina. Instead of rescheduling, she was offered and accepted a medication abortion.
As I understand it, she took the first pill, mifepristone, at the clinic, followed by misoprostol a couple of days later while at home in Georgia. Amber had a legal abortion. We also know that Amber began experiencing pain and other side effects after the abortion, but we don’t know the exact details since individual medical records aren’t public. We also don’t know how long she waited to seek medical attention after taking the mifepristone.
It’s important to remember that given the suspended Mifeprex REMS, abortion providers are no longer required to offer or to provide post-abortion care, effectively shifting the burden of care to the patient. Whether she fully understood what she was signing up for, Amber accepted personal responsibility for self-managing her abortion. She, and she alone, was entrusted to follow the instructions provided to her at the clinic. This information was also outlined in the Patient Consent she was required to sign before getting the pills (you can download the .pdf version of the Patient Consent at accessdata.fda.gov).
Meanwhile, here’s the text of the FDA-approved Mifepristone Patient Consent for your convenience:
PATIENT AGREEMENT FORM: Mifeprex (Mifepristone)
Healthcare Providers: Counsel the patient on the risks of Mifeprex*. Both you and the patient must sign this form.
Patient Agreement:
1. I have decided to take Mifeprex and misoprostol to end my pregnancy and will follow my provider’s advice about when to take each drug and what to do in an emergency.
2. I understand:
a. I will take Mifeprex on Day 1.
b. My provider will either give me or prescribe for me the misoprostol tablets which I will take 24 to 48 hours after I take Mifeprex.
3. My healthcare provider has talked with me about the risks including:
heavy bleeding
infection
ectopic pregnancy (a pregnancy outside the womb)
4. I will contact the clinic/office right away if in the days after treatment I have:
a fever of 100.4°F or higher that lasts for more than four hours
severe stomach area (abdominal) pain
heavy bleeding (soaking through two thick full-size sanitary pads per hour for two hours in a row)
stomach pain or discomfort, or I am “feeling sick”, including weakness, nausea, vomiting, or diarrhea, more than 24 hours after taking misoprostol
5. My healthcare provider has told me that these symptoms could require emergency care. If I cannot reach the clinic or office right away my healthcare provider has told me who to call and what to do.
6. I should follow up with my healthcare provider about 7 to 14 days after I take Mifeprex to be sure that my pregnancy has ended and that I am well.
7. I know that, in some cases, the treatment will not work. This happens in about 2 to 7 out of 100 women who use this treatment. If my pregnancy continues after treatment with Mifeprex and misoprostol, I will talk with my provider about a surgical procedure to end my pregnancy.
8. If I need a surgical procedure because the medicines did not end my pregnancy or to stop heavy bleeding, my healthcare provider has told me whether they will do the procedure or refer me to another healthcare provider who will.
9. I have the MEDICATION GUIDE for Mifeprex. I will take it with me if I visit an emergency room or a healthcare provider who did not give me Mifeprex so that they will understand that I am having a medical abortion with Mifeprex.
10. My healthcare provider has answered all my questions.
Patient Signature: Patient Name (print): Date:
The patient signed the PATIENT AGREEMENT in my presence after I counseled her and answered all her questions. I have given her the MEDICATION GUIDE for Mifeprex.
Provider’s Signature: Name of Provider (print): Date:
After the patient and the provider sign this PATIENT AGREEMENT, give 1 copy to the patient before she leaves the office and put 1 copy in her medical record.

Going to the Emergency Room
According to RealClearHealth.com, Amber Thurman’s symptoms included “uterine tenderness and odor, low blood pressure, [and] elevated white cell count” when she arrived at the hospital, all of which indicate sepsis. Now, her twins were already aborted, so she didn’t need another abortion (so Georgia abortion law isn’t in play here at all).
Amber did, however, need a D&C to clean out the infected tissue remaining from the incomplete abortion. For whatever reason, her doctors didn’t recognize the urgency of the situation until it was too late. We don’t know if they were even informed she’d had a DIY abortion or whether they assumed she naturally miscarried. Nor do we know if Amber took the MEDICATION GUIDE (see item 9 in bold on the Patient Consent form above) with her. In fact, there’s a lot we don’t know.
What we do know is that operating on a sepsis patient can be very dangerous. According to the Cleveland Clinic …
“Sepsis is a life-threatening medical emergency caused by your body’s overwhelming response to an infection … [which response] causes extensive inflammation throughout your body that can lead to tissue damage, organ failure and even death. Many different kinds of infections can trigger sepsis, which is a medical emergency. The quicker you receive treatment, the better your outcome will be.”
Even if Amber was still pregnant when she arrived at the ER, she was experiencing a life-threatening medical emergency and an abortion would have been fully justified under Georgia law.
My friend, Dr. Davis, has been in this awful situation many times and she tells me it’s very stressful for both provider and patient. With sepsis, the immune system often stops fighting the underlying infection and starts damaging normal healthy organs and bodily tissue, resulting in inflammation throughout the body. The risk of uterine perforation during a D&C is very high, which then creates an entirely new emergency.
Unfortunately, we don’t know why there was an 18 - 20 hour delay before Amber was on the operating table, but we do know that the surgeons were mid-hysterectomy when she flatlined. Amber, who was very very sick when she arrived at the ER, died on the operating table.
The truth is that Georgia’s abortion law didn’t even come into play in Amber’s situation. Even if it did, nothing in the statute prevented anyone from providing her with necessary medical care. In fact, it’s quite the contrary. Blaming the Georgia law is nonsensical, illogical, and done in bad faith.
The blame instead, if any is to be assigned, rests with the reckless FDA regulations Biden/Harris demanded in order to increase access to self-managed abortions, regardless of the cost to women. By suspending key components of the 2016 Mifeprex REMS, the current Administration knowingly shifted the burden for understanding the risks, following dispensing instructions, and being able and willing to seek emergency help in a timely manner from the provider to the patient.
This shift is fundamental to reducing the costs of abortion (about $150 online for pills) and increasing access to self-managed abortion. If doctors and nurses don’t have a duty to provide healthcare services beyond writing a script for a patient they don’t know, they certainly won’t be compensated by insurance companies, or even by Medicaid, for any additional services they provide. They, will, however, assume additional liability for those uncompensated-for services. Not a very enticing deal …
But, hey, that’s the nature of DIY.
When you shift burdens and responsibilities to the consumer, you get cheap and easy. The professionals are out, the laymen are in.
Candi Miller and her baby.
Candi Miller was a 41-year old married mother who’d been advised by her doctor to stop having children given her hypertension, lupus, and diabetes, among other comorbidities. All of these put her at extreme risk for pregnancy complications. Yet, she became pregnant again. According to ProPublica, Candi feared calling her doctor for guidance on how best to proceed since she erroneously believed that abortion is illegal in Georgia. So she decided to go it alone and just pray she wouldn’t get into trouble. This seems strange to me given that she had an ongoing relationship with a doctor who understood her specific history, but that wasn’t questioned or explored in the article.
As with Amber Thurman, we don’t know how far along Candi was, but we do know that she ordered abortion pills online through the website AidAccess.org. We also don’t know their origin, i.e. where they were manufactured and how they arrived in the United States.
It’s also unclear whether she was informed about the FDA’s explicit warning against buying mifepristone online since that’s not on the Patient Consent form.
Here’s an excerpt from the FDA’s website on buying pills online:
FDA Does Not Recommend Buying Mifepristone Online
Mifepristone prescribed under the Mifepristone REMS Program will be dispensed to you by your health care provider (or someone under the supervision of your health care provider), or by a pharmacy to which your health care provider has submitted your prescription. You can ask your health care provider whether they are certified in the Mifepristone REMS Program (or working under the supervision of someone who is). The FDA does not recommend purchasing mifepristone outside of the Mifepristone REMS Program – e.g. buying it online or personally transporting it from a foreign country. If a person does so, they would be bypassing important safeguards specifically designed to protect their health. Prescription medicines that are approved for use in the United States have been reviewed for safety, effectiveness, and quality by the FDA, and are subject to FDA-regulated manufacturing controls, including inspection of manufacturing facilities. Generally, prescription medicines purchased from foreign sources are not the FDA-approved versions. The FDA does not have regulatory oversight of prescription medicines from outside the legitimate U.S. drug supply chain; therefore, the FDA cannot ensure the safety, effectiveness, or quality of those medications.
To learn more about buying drugs safely, please see BeSafeRx: Your Source for Online Pharmacy Information.
Given her medical history, Candi never should have been prescribed chemical abortion pills. She should have been immediately referred to her obstetrician (or another OBGYN) to evaluate her situation and determine whether her symptoms were manageable or whether they were life threatening in case of pregnancy or medical abortion.
But, she wasn’t.
Had Candi been advised to consult a doctor who, upon examination, determined in their sole medical discretion, that her pregnancy created a medical emergency (which is broadly defined in the Georgia statute above), having a surgical abortion would have been 100% legal. Imminent danger or death isn’t required for their to be a medical emergency.
But, she wasn’t.
Instead, Candi Miller legally self-aborted with pills she legally purchased online, despite the fact that the FDA strongly discourages the practice. And instead of experiencing a complete abortion, she writhed in pain for days. According to her son, Candi was terrified to seek help.
But, there was no factual or legal basis for her fear, was there? Her fear was a natural response to the nonstop messaging that gaslights and terrorizes women into believing falsehoods about abortion laws.
During Candi Miller’s autopsy, the coroners found the partial remains of her aborted child. They also found a lethal combination of pain killers, including fentanyl. Her family is unsure where she obtained the fentanyl. Fentanyl is an FDA-approved Class II narcotic for exclusive use as an analgesic. It should only be used pursuant to a prescription and under close supervision of a physician to ensure the patient’s safety. You can read more about fentanyl on the Drug Enforcement Administration’s website.
Had Candi been armed with accurate information about her abortion, she would be alive today.
Make no mistake, abortion advocates climb into the bully pulpit and prey on women’s vulnerability by telling them the “mean bad people” on the right are so “anti-woman” they’ll do anything to “strip them of their rights” and keep them in the kitchen, barefoot and pregnant. And, that’s about as specific as they get. No evidence provided, just a healthy dose of ridiculous, nonsensical lies.
SIDEBAR » As I’ve been researching this issue, I came to understand that it’s never really been about women, their bodies, or “reproductive freedom.” It’s always been about power, women and their safety be damned. The lengths to which abortion advocates (particularly via the legal system) go to remove safeguards that protect the health of pregnant women, children, and teenagers seeking abortions is mind-boggling. More on that later.
But its all done in the name of access and empowering women, so it’s good, right?
Since abortion is the only medical procedure deemed successful when another human dies, it’s paramount to remove any barriers to its success. But, I’m confused. If abortion is healthcare, why don’t we insist it be regulated it as such?
Pause for a moment and ask yourself …
Why does the pro-choice lobby intentionally make pregnant women feel unsafe and incapable of receiving medical help for complications from a 100% legal self-managed abortion?
Who exactly is the object of their protests?
Who exactly is their beneficiary?
There’s a lot of smoke coming from this fire.

RIP Amber and Your Twins, and Candi and Your Child
Amber Marshall and Candi Miller died from well-known risks of legal medication abortion.
The changes in dispensing protocols that gave rise to self-managed abortion were implemented 14 months before Roe v. Wade was overturned. As discussed above, these revised requirements shifted the burden of care from providers to pregnant women having self-managed abortions. In the event of post-abortive side effects, complications, or other irregularities, the woman have the authority and responsibility to seek the proper and timely care as identified on the Patient Consent form and the black-box warning.
Any delay is on the patient, not the doctors and not the law.
And all of this was done by design.
CONCLUSION #6:
Amber Thurman and Candi Marshall died from well-known risks of chemical abortion. Nothing in Georgia law prevented them from receiving any and every type of medical care required to treat their conditions. In fact, Georgia physicians are expressly authorized by Georgia law to provide life-saving care to any pregnant, or formerly pregnant, woman experiencing a medically futile pregnancy or medical emergency.

My Body, My Choice
Self-managed abortion provides women with the highest level of personal autonomy, agency, and decision-making power over her body, and the one growing inside of it, in all of human history.
She, and she alone, has irreducible power to make the choice to have an abortion on her own terms, in her own timing, and at her desired location. Her body, her choice. Easy access, no hurdles. After all, medication abortion is extremely safe and effective, even safe than taking Tylenol.
But choices have consequences.
And with autonomy comes responsibility.
So, don’t forget to read the fine print. The devil is always in the details.
Wrapping it Up
Is ProPublica’s claim that, but for Georgia’s abortion law, Amber and Candi would be alive today true?
Let’s review what we’ve learned.
Both Amber Thurman and Candi Miller had legal self-managed medication abortions and both women died from complications arising from those abortions.
More than a year before Roe v. Wade was overturned, the Biden/Harris Administration suspended key elements of the mifepristone Risk Evaluation and Mitigation Strategies (REMS) clearing the way for mifepristone-misoprostol to be prescribed online and delivered through the mail.
The Biden/Harris Administration celebrates its decision to withdraw the in-person examination and dispensing protocols established in the 2016 REMS since it had the intended effect: legalizing self-managed abortion nationwide.
As of April 2021, self-managed abortion is legal, easy-to-obtain, and widely available in all 50 states.
Georgia abortion law expressly authorizes doctors to perform an abortion for pregnant women experiencing a medical emergency. Georgia law also expressly releases women who have abortions from any civil or criminal liability, whether the abortion is self-managed or performed by a doctor.
Amber Thurman and Candi Marshall died from well-known risks of chemical abortion. Nothing in Georgia law prevented either of them receiving any necessary medical care required to treat their conditions. Indeed, Georgia physicians are expressly authorized by Georgia law to provide life-saving care to pregnant women and post-abortive women experiencing a medically futile pregnancy or medical emergency.
Pro-Publica’s Claim is False
ProPublica didn’t prove anything beyond its own bias.
Not only did their articles fail to make their claim, they failed to establish even an attenuated causal link between Georgia’s abortion law and Amber and Candi’s 100% legal, but incomplete, self-managed abortions which caused their deaths.
The blame, if any is to be assigned, rests with President Biden and Vice President Harris for intentionally suspending key safeguards in the 2016 Mifeprex REMS for the sole purpose of opening the market for mail-order abortion, without regard for human toll in physical and emotional suffering and loss of life.
Final Thoughts
Lying to women about the risks of chemical abortion (or surgical abortion) isn’t empowering, it’s dehumanizing, demoralizing, and deadly.
Consider this case Exhibit A for my proposition.
Five people are dead: Amber, Candi, and their three unborn children.
Amber’s young child is orphaned.
Candi’s husband is widowed.
Candi’s children lost their mother.
And this is just the short list of immediate relations.
… but the only thing ProPublica has to say is Orange Man Bad.
This isn’t journalism.
This is a gross insult to women, their intelligence, and their misplaced reliance on the abortion movement’s commitment to tell them the truth.
But ProPublica, you already know that …

As John Adams famously said, “facts are stubborn things.”
In every situation there are good facts and bad facts. Everyone deserves ALL the facts, ALL the time, on ALL matters relevant to their lives, but especially when a women plans to take medically-classified dangerous drugs that will certainly kill their unborn child/children, but just might kill them too.
—-
I write in service to the truth, the whole truth, and nothing but the truth … without it, there is no choice, just coercion.
xo,
Kelley
September 25, 2024
P.S. Thank you for following and supporting my work.
Excellent article! You did the job that journalists should do. If they did, without the bias and activism that pervades today's media, their reporting would be much different than what we read and see. Thank you for your great research and presentation! I hope journalists will learn from it.
What a well researched and written piece!